Health:Hypertension

Hello my fellow steemians, welcome to my new post in health series where i will be discussing common health problems prevalent in our communities.
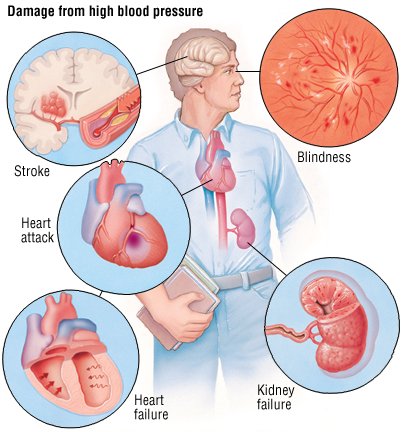
Today we will be discussing about Hypertension- 'Hypertension is a condition in which arterial BP is chronically elevated. BP occurs within a continuous range, so cutoff levels are defined according to their effect on patients’ risk.'
AETIOLOGY
In more than 95% of cases, a specific underlying cause of hypertension cannot be found. Such patients are said to have essential hypertension. The pathogene- sis of this is not clearly understood. Many factors may contribute to its development, including renal dys- function, peripheral resistance vessel tone, endothelial dysfunction, autonomic tone, insulin resistance and neurohumoral factors. Hypertension is more common in some ethnic groups, particularly Black Americans and Japanese, and approximately 40–60% is explained by genetic factors. Important environmental factors include a high salt intake, heavy consumption of alco- hol, obesity, lack of exercise and impaired intrauterine growth. There is little evidence that ‘stress’ causes hypertension.

CAUSES OF SECONDARY HYPERTENSION
.alcohol
.obesity
.Pregnancy (pre-eclampsia)
renal disease
• Renal vascular disease
• Parenchymal renal disease, particularly glomerulonephritis • Polycystic kidney disease
Endocrine disease
• Phaeochromocytoma
• Cushing’s syndrome
• Primary hyperaldosteronism (Conn’s syndrome) • Glucocorticoid-suppressible hyperaldosteronism • Hyperparathyroidism
• Acromegaly
• Primary hypothyroidism
• Thyrotoxicosis
• Congenital adrenal hyperplasia due to 11-β-hydroxylase
or 17α-hydroxylase deficiency
• Liddle’s syndrome
• 11-β-hydroxysteroid dehydrogenase deficiency
drugs
• e.g. Oral contraceptives containing oestrogens, anabolic steroids, corticosteroids, NSAIDs, carbenoxolone, sympathomimetic agents
Coarctation of the aorta
HYPERTENSION: INVESTIGATION OF ALL PATIENTS
• Urinalysis for blood, protein and glucose
• Blood urea, electrolytes and creatinine
Hypokalaemic alkalosis may indicate primary
hyperaldosteronism but is usually due to diuretic therapy
• Blood glucose
• Serum total and HDL cholesterol
• 12-lead ECG (left ventricular hypertrophy, coronary artery
disease)
HYPERTENSION: investigation of selected patients
• Chest X-ray: to detect cardiomegaly, heart failure, coarctation of the aorta
• Ambulatory BP recording: to assess borderline or ‘white coat’ hypertension
• Echocardiogram: to detect or quantify left ventricular hypertrophy
• Renal ultrasound: to detect possible renal disease
• Renal angiography: to detect or confirm presence of renal
artery stenosis
• Urinary catecholamines: to detect possible
phaeochromocytoma
• Urinary cortisol and dexamethasone suppression test: to
detect possible Cushing’s syndrome
• Plasma renin activity and aldosterone: to detect possible
primary aldosteronism
BENEFIT OF ANTIHYPERTENSIVE DRUG THERAPY
‘Diuretics or β-blockers have been shown to reduce the risk of coronary heart disease by 16%, stroke by 38%, cardiovascular death by 21% and all causes of mortality by 13%. The effects of ACE inhibitors and calcium antagonists are similar. NNTB varies greatly according to the absolute baseline risk of cardiovascular disease.’
HYPERTENSION IN OLD AGE
• Prevalence: affects more than half of all people over the age of 60 (including isolated systolic hypertension).
• risks: hypertension is the most important risk factor for MI, heart failure and stroke in older people.
• Benefit of treatment: absolute benefit from antihypertensives is greatest in older people (at least up to age 80 years).
• target BP: similar to that for younger patients.
• tolerance of treatment: antihypertensives are tolerated as
well as in younger patients.
• drug of choice: low-dose thiazides, but in the presence
of coexistent disease (e.g. gout, diabetes) other agents may be more appropriate.
OPTIMAL TARGET BLOOD PRESSURES DURING ANTIHYPERTENSIVE TREATMENT: BHS GUIDELINES
Clinic measurements
no diabetes
< 140/85
diabetes
< 130/80
mean day-time ambulatory < 130/80 < 130/75 or home measurement
n.B. Both systolic and diastolic values should be attained.
Reference and Sources:- Davidson's principle of medicine 26/e

Thankyou for reading my post.
With love
@anilmehta00

@originalworks
The @OriginalWorks bot has determined this post by @anilmehta00 to be original material and upvoted it!
To call @OriginalWorks, simply reply to any post with @originalworks or !originalworks in your message!
To nominate this post for the daily RESTEEM contest, upvote this comment! The user with the most upvotes on their @OriginalWorks comment will win!
For more information, Click Here!
This post recieved an upvote from minnowpond. If you would like to recieve upvotes from minnowpond on all your posts, simply FOLLOW @minnowpond
This post recieved an upvote from minnowpond. If you would like to recieve upvotes from minnowpond on all your posts, simply FOLLOW @minnowpond
This post has received a 0.03 % upvote from @boomerang thanks to: @anilmehta00
@boomerang distributes 100% of the SBD and up to 80% of the Curation Rewards to STEEM POWER Delegators. If you want to bid for votes or want to delegate SP please read the @boomerang whitepaper.
Resteemed your article. This article was resteemed because you are part of the New Steemians project. You can learn more about it here: https://steemit.com/introduceyourself/@gaman/new-steemians-project-launch
@anilmehta00 got you a $1.42 @minnowbooster upgoat, nice! (Image: pixabay.com)
Want a boost? Click here to read more!