CLINICAL CASE
WOMAN OF 93 YEARS SYNTHETIC WITH DISNEAD OF MEDIUM TO SMALL EFFORTS THAT PROGRESSES TO ORTOPNEA, EPISODES OF NON-NURTURAL PAROXYSIS DISSAYS AND EDEMS IN THE LOWER LIMBS OF AT LEAST 4 WEEKS OF EVOLUTION, ASCENDING. THE PHYSICAL EXAMINATION WAS EVIDENCED BILATERAL CREPSANTS, YUGULAR INGURGITATION AND MULTIFOCAL PANSISTOLIC BREATH.
A TRANSTORACICAL ECOCARDIOGRAM WHICH SHOWED THE NORMOCONTRACTORY LEFT VENTRICLE, RIGHT VENTRICLE (VD) SLIGHTLY DILATED AND HYPOQUINETIC AND A LIGHT TRICUSTIC INSUFFICIENCY SHOWED
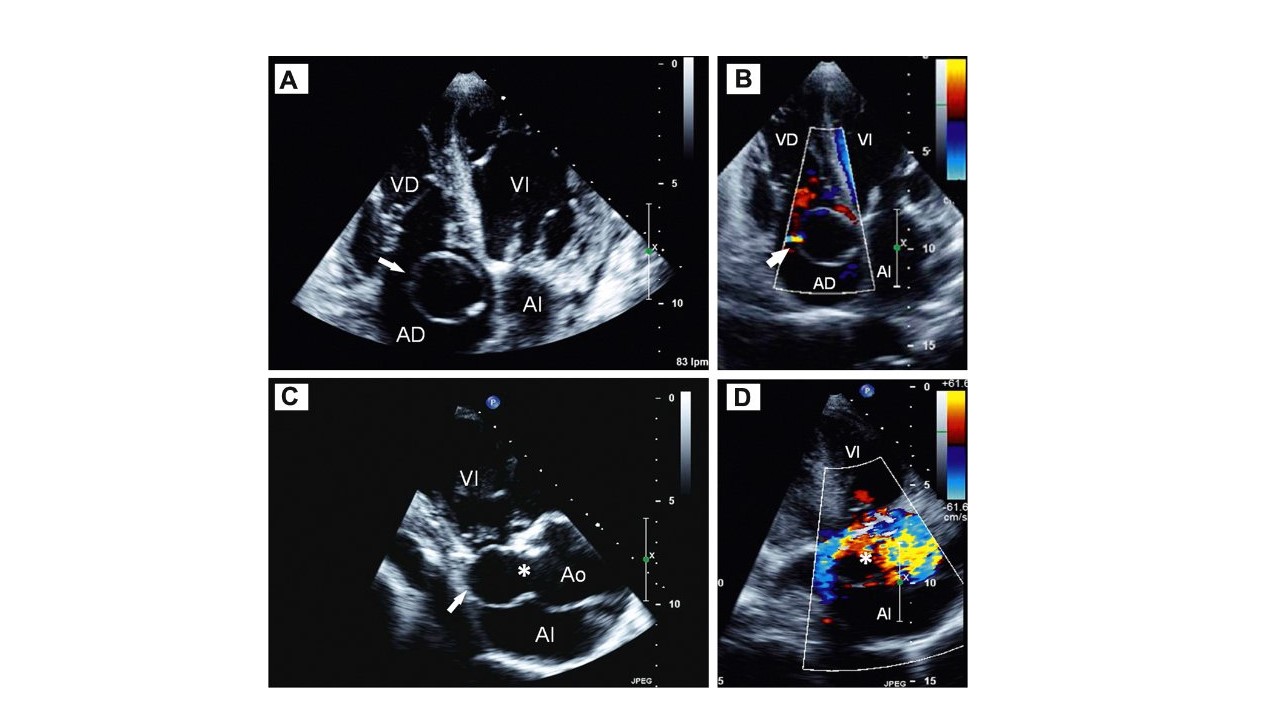
In the apical plane of four chambers, an annular, very well defined image was observed, floating inside the right atrium (AD) (arrow, figure A)

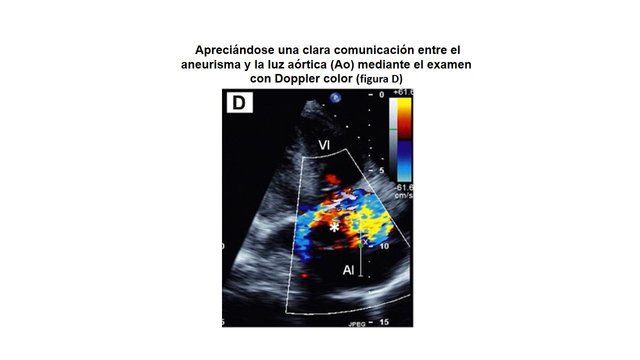
A careful rotation of the transducer towards an apical view of three chambers revealed that the infrequent annular image in AD corresponded to a large aneurysm of the non-coronary sinus of Valsalva (arrow, figure C)
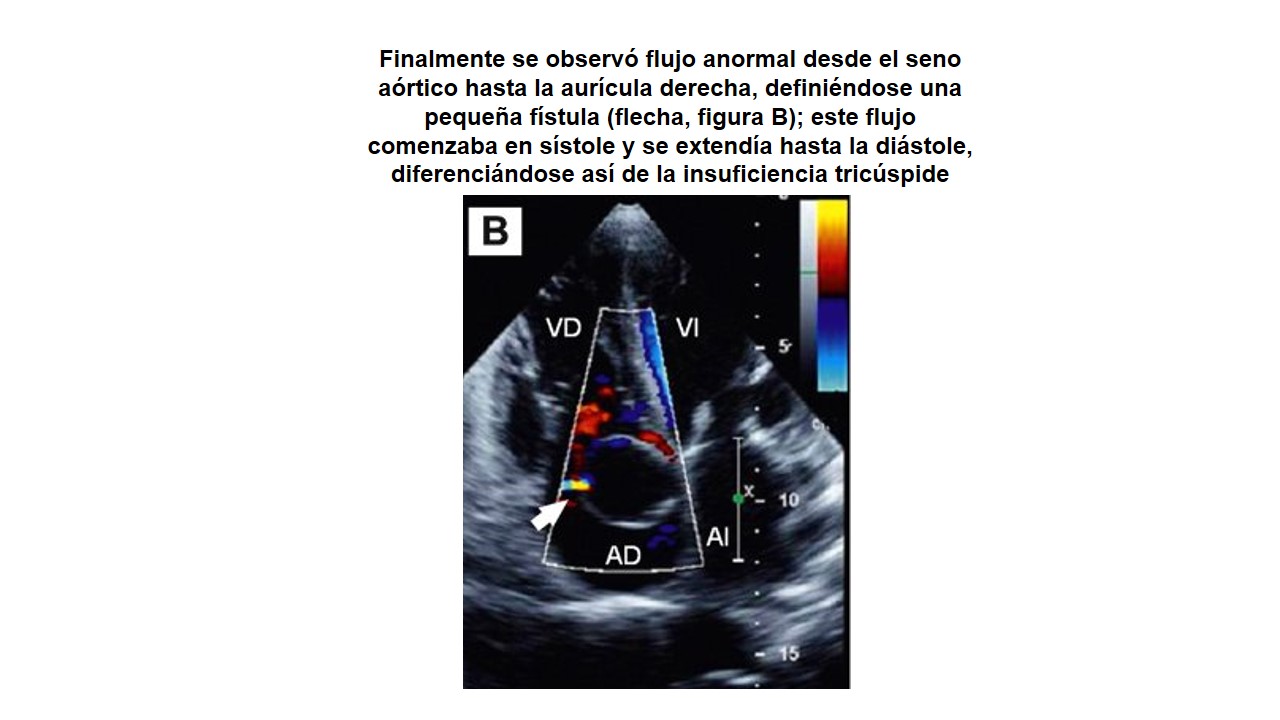
A clear communication between the aneurysm and aortic lumen (Ao) is appreciated by color Doppler examination (Figure D)
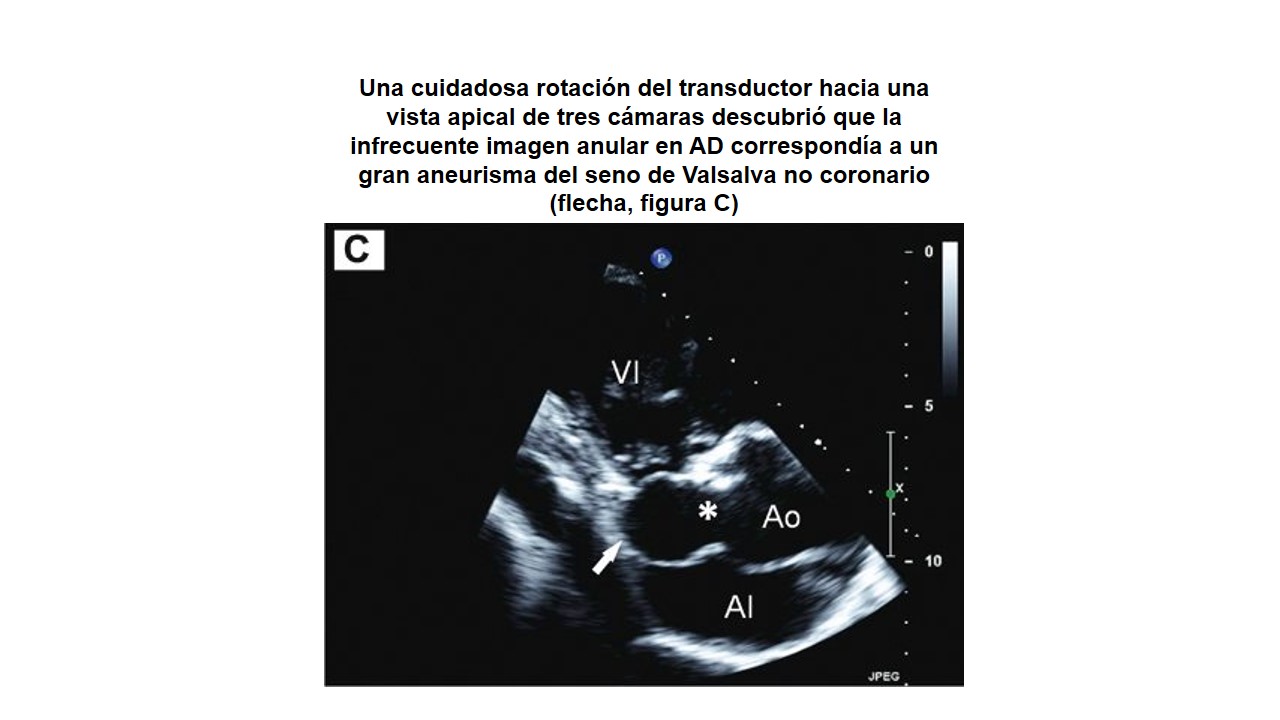
Finally, abnormal flow was observed from the aortic sinus to the right atrium, defining a small fistula (arrow, figure B); this flow started in systole and extended until the diastole, differentiating itself from the tricuspid insufficiency
The final clinical diagnosis was heart failure due to overload of the right ventricle secondary to left-right shunt.
The treatment of choice for sinus aneurysms of Valsalva that fistulize other cardiac chambers is surgical correction, but given the patient's advanced age, any aggressive treatment was dismissed, and she was discharged after compensating for her heart failure.