Diabetes insipidus
 Diabetes insipidus (die-uh-BEE-teze in-SIP-uh-dus) is an uncommon disorder characterized by intense thirst, despite the drinking of fluids (polydipsia), and the excretion of large amounts of urine (polyuria). In most cases, it's the result of your body not properly producing, storing or releasing a key hormone, but diabetes insipidus can also occur when your kidneys are unable to respond properly to that hormone. Rarely, diabetes insipidus can occur during pregnancy (gestational diabetes insipidus).
Diabetes insipidus (die-uh-BEE-teze in-SIP-uh-dus) is an uncommon disorder characterized by intense thirst, despite the drinking of fluids (polydipsia), and the excretion of large amounts of urine (polyuria). In most cases, it's the result of your body not properly producing, storing or releasing a key hormone, but diabetes insipidus can also occur when your kidneys are unable to respond properly to that hormone. Rarely, diabetes insipidus can occur during pregnancy (gestational diabetes insipidus).
You may assume diabetes insipidus and diabetes mellitus — the more common form of diabetes involving blood sugar — are related. Although the disorders share a name and have some common signs, diabetes mellitus (type 1 and type 2) and diabetes insipidus are unrelated.
Treatments are available to relieve your thirst and normalize your urine output.
SYMPTOMS
The most common signs and symptoms of diabetes insipidus are:
Extreme thirst
Excretion of an excessive amount of diluted urine
Depending on the severity of the condition, urine output can range from 2 quarts (about 2 liters) a day if you have mild diabetes insipidus to 21 quarts (about 20 liters) a day if the condition is severe and if you're drinking a lot of fluids. In comparison, the average urine output for a healthy adult varies, but is in the range of 1.6 to 2.6 quarts (about 1.5 to 2.5 liters) a day.
Other signs may include needing to get up at night to urinate (nocturia) and bed-wetting.
Infants and young children who have diabetes insipidus may have the following signs and symptoms:
Unexplained fussiness or inconsolable crying
Unusually wet diapers
Fever, vomiting or diarrhea
Dry skin with cool extremities
Delayed growth
Weight loss
When to see a doctor
See your doctor immediately if you notice the two most common signs of diabetes insipidus: excessive urination and extreme thirst.
CAUSES
Diabetes insipidus occurs when your body can't regulate how it handles fluids. Normally, your kidneys remove excess body fluids from your bloodstream. This fluid waste is temporarily stored in your bladder as urine, before you urinate. When your fluid regulation system is working properly, your kidneys make less urine when your body water is decreased, such as through perspiration, to conserve fluid.
The volume and composition of your body fluids remain balanced through a combination of oral intake and excretion by the kidneys. The rate of fluid intake is largely governed by thirst, although your habits can increase your intake far above the amount necessary. The rate of fluid excreted by your kidneys is greatly influenced by the production of anti-diuretic hormone (ADH), also called vasopressin.
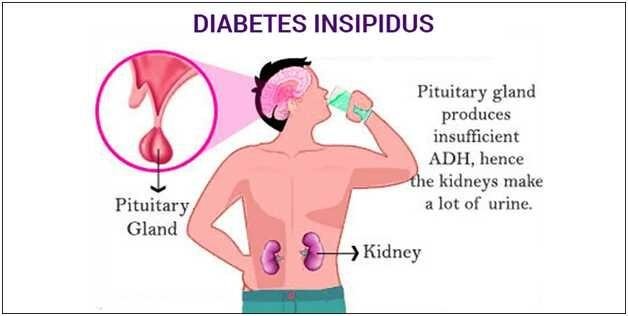
Your body makes ADH in the hypothalamus and stores the hormone in your pituitary gland, a small gland located in the base of your brain. ADH is released into your bloodstream when your body starts to become dehydrated. ADH then concentrates the urine by triggering the kidney tubules to release water back into your bloodstream rather than excreting as much water into your urine.
The way in which your system is disrupted determines which form of diabetes insipidus you have:
Central diabetes insipidus. The cause of central diabetes insipidus in adults is usually damage to the pituitary gland or hypothalamus, most commonly due to surgery, a tumor, an illness (such as meningitis), inflammation or a head injury. For children, the cause is often an inherited genetic disorder. In some cases the cause is unknown. This damage disrupts the normal production, storage and release of ADH.
Nephrogenic diabetes insipidus. Nephrogenic diabetes insipidus occurs when there's a defect in the kidney tubules — the structures in your kidneys that cause water to be excreted or reabsorbed. This defect makes your kidneys unable to properly respond to ADH. The defect may be due to an inherited (genetic) disorder or a chronic kidney disorder. Certain drugs, such as lithium and demeclocycline (a tetracycline antibiotic), also can cause nephrogenic diabetes insipidus.
Gestational diabetes insipidus. Gestational diabetes insipidus occurs only during pregnancy and when an enzyme made by the placenta — the system of blood vessels and other tissue that allows the exchange of nutrients and waste products between a mother and her baby — destroys ADH in the mother.
Primary polydipsia. This condition — also known as dipsogenic diabetes insipidus or psychogenic polydipsia — can cause excretion of large volumes of dilute urine. Rather than a problem with ADH production or damage, the underlying cause is intake of excessive fluids. Prolonged excessive water intake by itself can damage the kidneys and suppress ADH, making your body unable to concentrate urine. Primary polydipsia can be the result of abnormal thirst caused by damage to the thirst-regulating mechanism, situated in the hypothalamus. Primary polydipsia can also be caused by mental illness.
In some cases of diabetes insipidus, doctors never determine a cause.
RISK FACTORS
Nephrogenic diabetes insipidus that's present at or shortly after birth usually has a genetic cause that permanently alters the kidneys' ability to concentrate the urine. Nephrogenic diabetes insipidus usually affects males, though women can pass the gene on to their children.
COMPLICATIONS
Dehydration
Except for primary polydipsia, which causes you to retain too much water, diabetes insipidus can cause your body to retain too little water to function properly, and you can become dehydrated. Dehydration can cause:
Dry mouth
Muscle weakness
Low blood pressure (hypotension)
Elevated blood sodium (hypernatremia)
Sunken appearance to your eyes
Fever
Headache
Rapid heart rate
Weight loss
Electrolyte imbalance
Diabetes insipidus can also cause an electrolyte imbalance. Electrolytes are minerals in your blood — such as sodium and potassium — that maintain the balance of fluids in your body. Electrolyte imbalance can cause symptoms, such as:
Fatigue or lethargy
Irritability
Nausea
Loss of appetite
Muscle pains