Elbow fracture reduction maneuver in children
In the following post I will show one of the fundamental techniques in the area of pediatrics. Which represents one of the most common pediatric orthopedic injuries in children, also known as radial head subluxation or painful pronation. This mild injury is usually painful for our little ones, usually is the result of a sudden twist of the elbow, usually seen more often in preschoolers between 1 and 4 years.
It is very predominant in girls, and on the left side, it is supposed to be because usually the child's caregiver is right-handed and he holds the child's left hand with his right hand as they walk.
In the medical area we know this injury as the displacement of the annular ligament, which consists of an elastic band that holds the bone structure of the radius and ulna together at elbow level. When a child's arm is pulled tightly, this ligament is displaced, becoming trapped between the bone and the elbow joint.

Public domain piqsel
In turn, there is no fracture as such of the bone structure, only displacement of the structure that holds them fixed, which is why it is called subluxation.
Anatomy
Our upper limbs consist of long and short bones joined together by various joints. This portion of our body is made up of the humerus, radius, and ulna joined by the joint called the elbow, which is described below.
The elbow impresses at first sight a simple joint with a function similar to a hinge, however it is not, it is a complex structure that gives stability and movement to this extremity.
The elbow is composed of 3 joints, humerus-radial, humerus-ulnar and the radio-ulnar, all grouped in the same joint capsule, also includes a series of ligaments and muscles (triceps brachial, biceps brachial, brachioradial, short supinator, pronator round and square) together allows the limb movement of extension, flexion, supination and pronation.
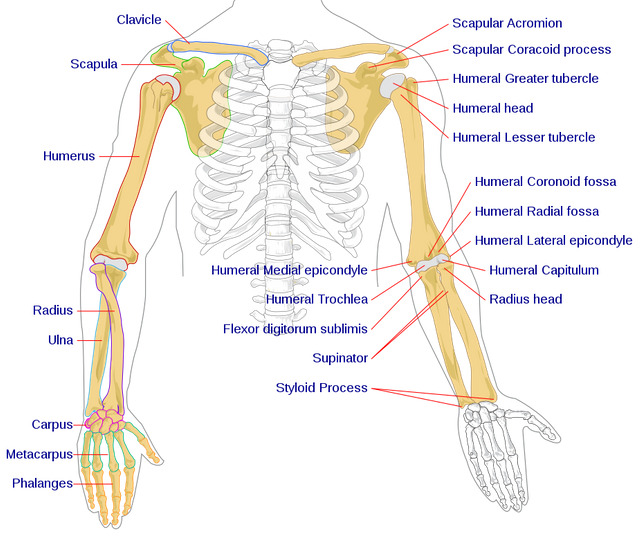
Human arm bones diagram. Public domain licensed CC BY-SA 3.0. Author: LadyofHats Mariana Ruiz Villarreal
Mechanism of the injury
The classic mechanism consists of a longitudinal or axial traction on an extended elbow and a pronounced forearm. This injury usually occurs when an adult (caregiver) grabs the child by the hand or wrist while the child is attached to an object, on the floor or suspended by the arm.
Other situations in which this injury occurs are when the adult lifts the child from the bed, floor, or chair, pulls the child's hand during a walk in a tantrum, or in situations where the child tries to free himself or herself from the caregiver and the caregiver holds the child's hand, even when the adult tries to prevent the child from falling and holding the child's hand.
Physiopathology
The injury affects the elbow region, where the ring ligament representing a thick band around the neck and head of the radius facilitates pronation and supination movements. The injury causes the head of the radius to dislocate relatively from its joint with the ulnar and capitellum of the humerus while the forearm is in pronation.
The ring ligament then slips to the lateral edge and becomes trapped between the radius and humerus, with the forearm remaining in the pronation position as a result of the trapped ligament.

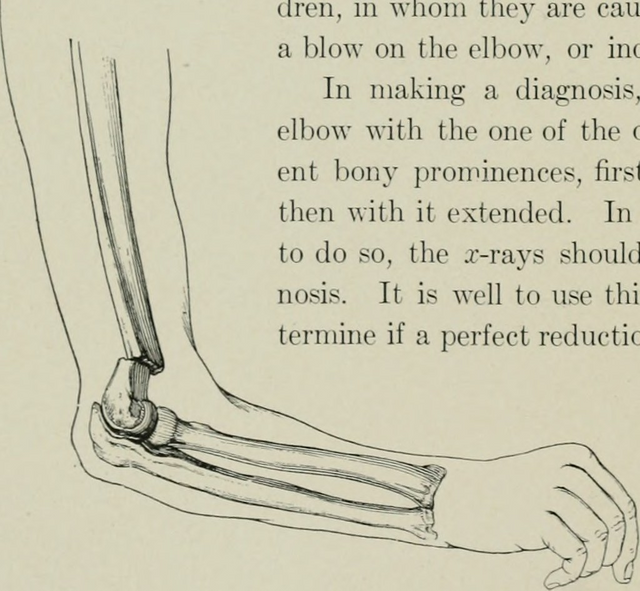
Left elbow extended and flexed from wikipedia. Public domain CC BY-SA 3.0
This pathology is painless as long as the forearm remains in the pronation position since trying to bring it into the supination position generates pain. However, the way to correct this injury is to bring the forearm into the supination position since this would spontaneously return the annular ligament to its anatomical place.
X-rays are not required unless another trauma is suspected involving the bony part. The subluxation of the radius head is often spontaneously reduced during placement for x-ray.
How to perform the maneuver
Any child with an inability to use the partially bent elbow, pronounced forearm and adducted forearm compatible with radius head subluxation should be reduced. In some situations physicians may be hesitant to repeat the reduction maneuver multiple times, especially those cases where the arm is not able to perform normal arm movements within 15 minutes of reduction, even though they are confident that the reduction was clinically satisfactory.
However, if the x-rays are normal, with a clinical history and physical examination compatible with subluxation, the maneuver should be repeated again.
Contraindications
The presence of edema (increased volume) ecchymosis, pain in an area other than the head of the radius, suspected fracture or a mechanism of injury not compatible with subluxation of the head of the radius should be x-rayed first to rule out the presence of a fracture or other adjacent injury.
Manoeuvre
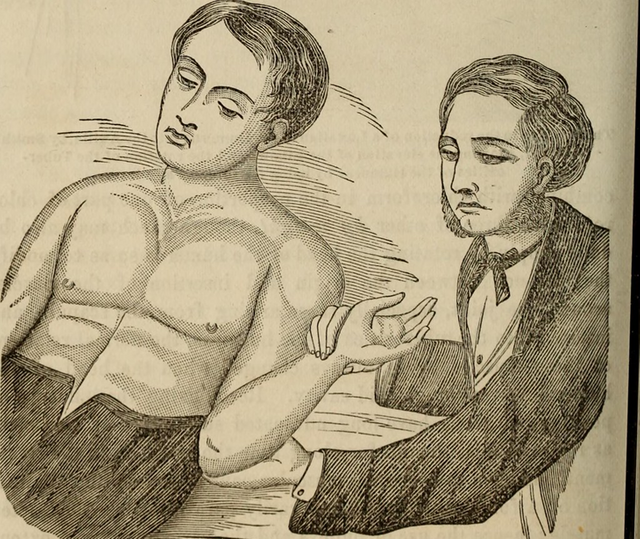
It should first be explained to the patient, and in this case to the parent or representative of the minor, so that informed consent can be obtained.
The patient should be placed on the legs of the parent or caregiver or an alternative in a supine position on an examination table or gurney.
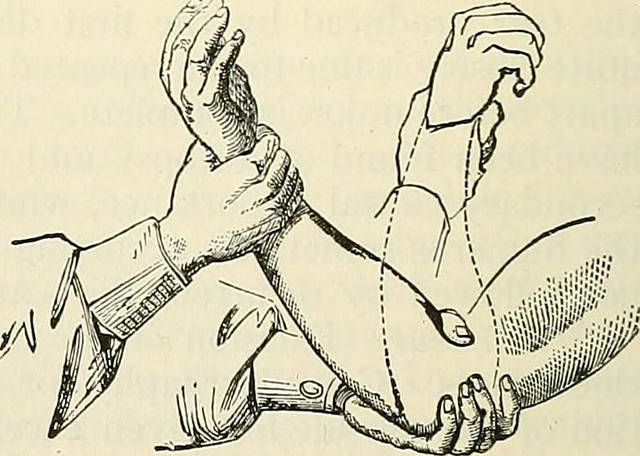
Place the non-dominant hand on the child's elbow with the thumb on the head of the radius, allowing the traditional reduction "click" to be felt.
Gently hold the child's wrist with the dominant hand. Apply distal traction while supine the forearm, followed by elbow flexion.
You may feel a "click" as the head of the radius is reduced. If not, flex the forearm until the hand is vertical.
Once the click is satisfactorily felt and you feel confident about the reduction, wait 5 to 15 minutes to repeat the scan. Usually the child cries at the end of the maneuver, almost always for a moment and as the child feels more comfortable he or she will go back to using the arm.
{kind=link}
{kind=link}
This freedom of use can be made faster if the child is encouraged to use his arm, by giving prizes, sweets and so on.
Confirmation
The child should make uninhibited use of the forearm within 30 minutes. If not, the diagnosis of subluxation should be reconsidered.
Alternative diagnoses may include clavicle fracture, distal humerus, osteomyelitis, radial head fracture, and stress fractures during the procedure. Explore the elbow joint for signs of trauma.
We should order an x-ray to rule out any type of injury. Full recovery may take about 24 to 48 hours, if this time is extended, to rule out another underlying injury.
Care after the maneuver
X-rays, immobilizations, splints, pain medications, and orthopedic follow-up are not necessary if the subluxation is reduced and the child uses his or her arm without problems. It is recommended that the parent and/or caregiver be instructed on the mechanism of the injury so that it does not recur and thus prevent future subluxations.
It is recommended that the child be evaluated by an orthopaedic surgeon if reduction is not successful. Immobilize the arm until the child is evaluated by an orthopedic specialist, as immobilization will help decrease pain in conjunction with anti-inflammatory analgesics while further studies are performed.
Sources:

steemSTEM is a project of the chain of blocks that supports the scientific content in different areas of science. If you want to know more about this wonderful project you can join the server in discord
This article will be published at https://www.steemstem.io/
link
If you have any questions about any topic of medicine or present any disease you can comment the publication or write me in discord and I will attend you.
Dr. Ana EstradaI hope you enjoyed my content.
This post has been voted on by the SteemSTEM curation team and voting trail. It is elligible for support from @curie and @minnowbooster.
If you appreciate the work we are doing, then consider supporting our witness @stem.witness. Additional witness support to the curie witness would be appreciated as well.
For additional information please join us on the SteemSTEM discord and to get to know the rest of the community!
Thanks for having used the steemstem.io app and included @steemstem in the list of beneficiaries of this post. This granted you a stronger support from SteemSTEM.
Thank you very much @steemstem