Let's talk about the painful "biliary colic"
Pain, whatever its location and cause, represents a signal from our CNS that something is not right in our body, and needs to be fixed as soon as possible. This sensory perception can become unpleasant and disabling based on its intensity and location in the human body.
This sensation of pain is nothing more than a physiological response of sensitive nerve endings that when stimulated generate this response. It can present itself as acute, with abrupt onset, sudden and usually limited, while when it is pain it is chronic that persists over time and varies in intensity.
According to the presentation of the pain, it would make us orientate to the pathology that triggers it to be treated later and to alleviate the pain.
However, this article will develop a frequent topic in the general practitioner's office, who must know how to diagnose, treat and refer to a specialist for the total resolution of the pain.
Vesicular lithiasis is one of the growing digestive pathological entities in the last decade, being more frequent in women (probably due to the influence of estrogens), obese patients, hypertriglyceridemia, frequent use of some drugs (oral contraceptives, exogenous estrogens, antibiotics such as ceftriaxone among others) and special situations that generate the production of the same as hemolytic anemia, liver cirrhosis.

Public domain Pixabay
Gallbladder
There is a small portion called the bile ducts and it is of interest to bring them in, anatomically these ducts comprise the hepatic bile ducts, intra and extrahepatic bile ducts which include the common bile duct, cystic ducts and the fine gallbladder.
The intrahepatic bile duct is responsible for transporting bile made by the liver to the digestive tract. It is made up of the segmental canaliculi, so called because they come from the hepatic segments. The extra hepatic bile duct represents the union between the right and left hepatic bile ducts that pass to form a common duct called the common hepatic duct, which continues its journey when it joins with the cystic duct giving rise to the common bile duct with an approximate length of 6 to 7.5 mm in diameter.
The bile duct is directed down and in to contact with the wall of the second portion of the duodenum, where it joins the pancreatic duct and finally ends in the ampulla of Vater.
The cystic duct has its origin in the neck of the vesicle with a length between 0.5 to 4 cm, with multiple anatomical variations in this area receives its irrigation from the branches of the cystic artery.
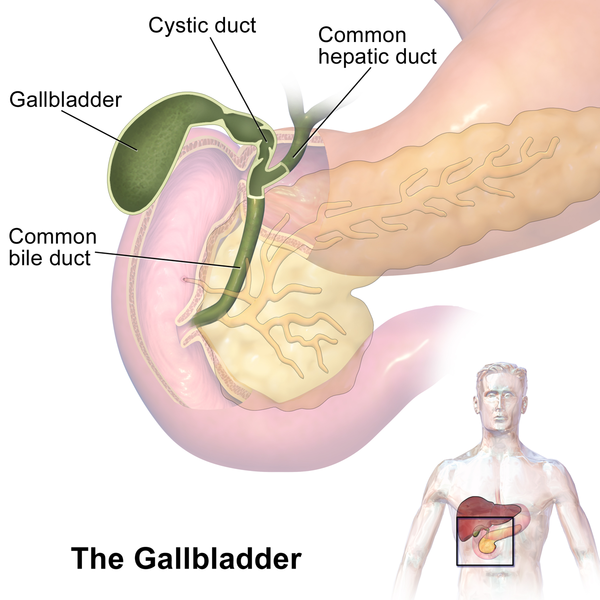
Gallbladder (organ). Public domain CC BY-SA 4.0. Author: BruceBlaus
The gallbladder has a pear-shaped, muscular-membranous composition. This sacular structure has an approximate length of 8 to 10cm, located in the cystic fossa, (between the square lobe of the liver and the tenth right costal arch). For its study the vesicle is divided into:
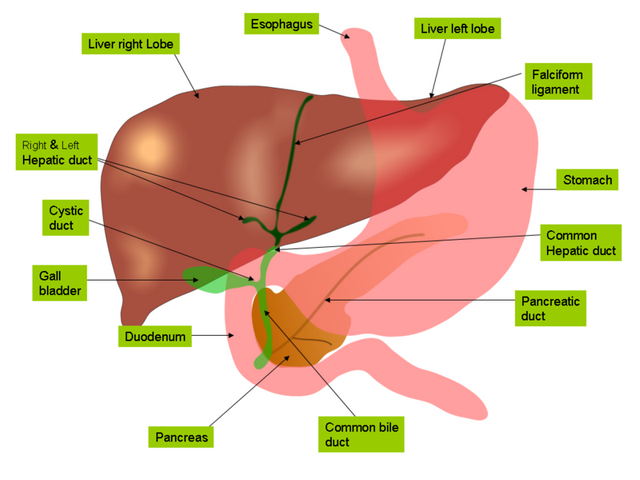
Anatomy of the biliary tree, liver and gall bladder. Public domain CC BY-SA 4.0. Author: Jiju Kurian Punnoose
Gallstones
Composition
Two types of bile duct stones have been described; cholesterol and pigment stones.
The cholesterol stones, occur more frequently around 80%, as its name indicates cholesterol compound, this occurs when it accumulates and concentrates in the bile at high doses. It is usually associated with obesity, hypertriglyceridemia, abundant weight loss in a short time (since cholesterol is excreted in an exaggerated way) drugs such as oral contraceptives, advanced age, women among others.
On the other hand, pigment stones are subdivided into black and ochre stones, where the former is more prevalent in the elderly or in cases of intravascular hemolysis. Ochre stones are usually associated with infectious processes such as parasitosis (lumbricoid acari).
Stones of mixed composition consisting of a calcium coating and a cholesterol centre have been found.
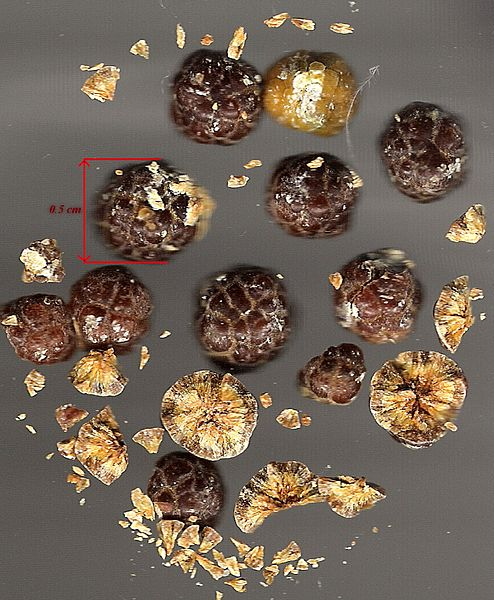
Gallstones from gall bladder. Public domain ional CC BY-SA 4.0. Author: Sacud
What's the problem?
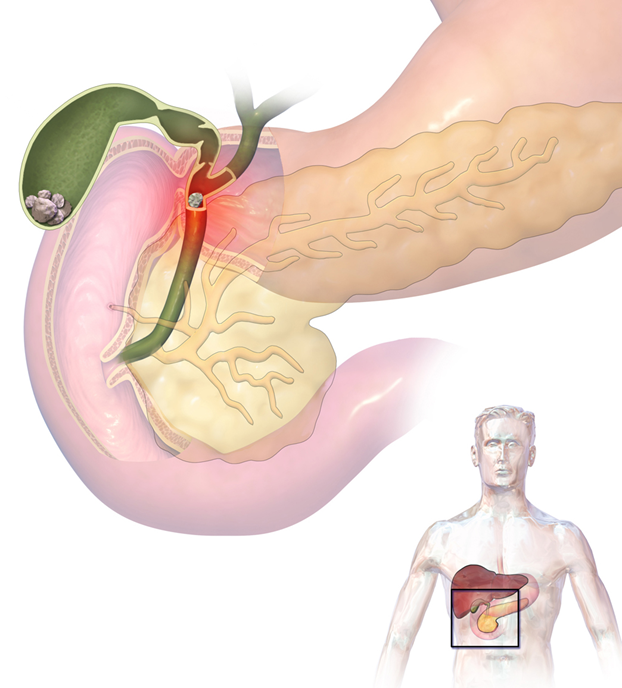
The physiopathology is not very clear, once the gallstone is formed which can be a single large or multiple small diameter, usually inside the gallbladder by a stimulus not very well described, (either excessive intake of large meals, rich in fat) able to stimulate the stone to its migration, output and direction to the bile ducts, generating an obstructive pattern that translates into colicky pain when this happens.
This obstructive pattern is the trigger in this pathology, i.e. the presence of gallstones in the vesicle backyard, causing first intense contraction and distension of the vesicle, which generates typical colic pain, and which in turn is capable of producing edema at the level of the vesicle wall and finally retention of bile fluids and vascular alteration (ischemia).
This obstruction is capable of causing an increase in intraluminal pressure and bacterial proliferation, favoring the passage of microorganisms to the portal and lymphatic circulation, which is why the patient may manifest fever. The germs mostly involved are intra-abdominal gram-negative, such as E. coli, Enterococcus Bacteroides among others.
Also the presence of the edema in the vesicle triggers an exaggerated release of phospholipase which is capable of converting lecithin into lysoselectin whose presence activates synthesis of arachidonic acid from phospholipids which leads to the activation of prostanglandins I2 and E2 giving way to the inflammatory process.
Finally, vascular alterations due to persistent obstruction for a long time are frequently observed due to ischemia caused by decreased blood flow, mainly in cystic vessels.
Clinical manifestations
Colic-type pain gradually located in the right hypochondrium or epigastric, which can radiate to the scapula or shoulder, is what defines this pathological entity.
Biliary colic can have a simple presentation, which appears 3 hours after the ingestion of copious food, usually of short duration, approximately 6 hours, which gradually subsides spontaneously or by the ingestion of analgesics.
While complicated biliary colic, resulting from an obstruction, is prolonged in duration and of greater intensity, it partially subsides with intravenous analgesics, may be accompanied by nausea, vomiting and even chills and fever, in severe cases of jaundice and sepsis (systemic infection).
Clinical signs:
On clinical abdominal examination, a resistance or hypersensitivity response to palpation in the right hypochondrium was generated, with a positive Murphy's sign, which translates into pain, followed by a short period of apnea, on deep palpation of the right costal ridge (area of the right hypochondrium gall bladder).
Diagnosis
{kind=link}
{kind=link}
{kind=link}
{kind=link}
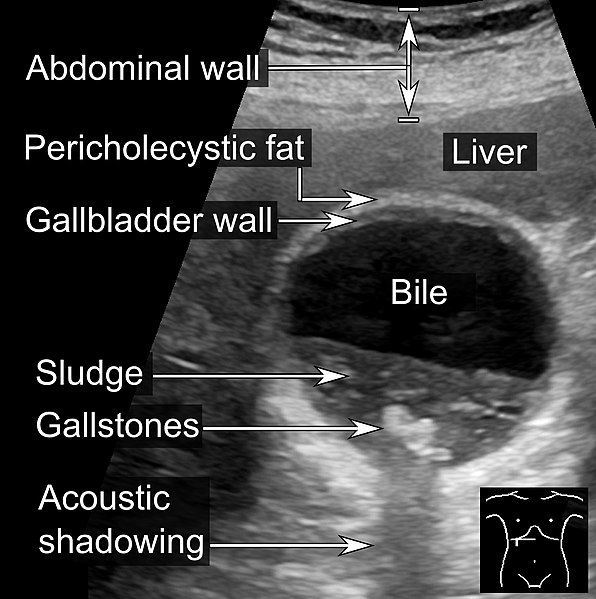
Abdominal ultrasound is the method of choice, when we suspect the presence of gallstones in the gallbladder, is a simple and inexpensive technique, does not offer reliable results and immediately. When we think that we are under the context of acute cholecystitis due to stones, there are ultrasound signs suggestive of it, such as; sonographic Murphy's sign, vesicular distension, thickening of the vesicular wall, double halo sign, among others.
Laboratory tests, in cases of simple biliary colic, no repercussions are observed in terms of liver function or the presence of leukocytosis (tests within normal parameters).
When we find ourselves in the presence of persistent biliary colic and we suspect that our patient is suffering from acute cholecystitis, it is frequent to observe moderate leukocytosis at the expense of neutrophils, discrete alteration of the hepatic profile, hyperbilirubinemia at the expense of direct leukocytosis, as well as elevation of inflammation mediating markers such as ESR and elevated CRP.
Other alternative studies are the Abdominal Magnetic Resonance, or the Abdominal Tomography.
Treatment
Medical treatment
Simple biliary colic; with good response to a low-fat diet, decreased grain intake, NSAID-type analgesia that can be oral or intravenous, and gastric protection. These patients should be referred to general surgery for subsequent surgical resolution.
Persistent biliary colic (acute cholecystitis); these patients deserve to be admitted to a hospital unit, absolute diet at least 24 hours or until the abdominal pain subsides.
Fluid therapy or parenteral hydration with physiological solution at 0.9% alternated with dextrose solution at 5%.
Parenteral electrolytes with calcium gluconate, magnesium sulfate and potassium chloride at 7.5% while the patient remains on the absolute diet.
Fixed intravenous analgesia at least 48 to 72 hours, NSAIDs with analgesic and anti-inflammatory action are useful and recommended.
Intravenous antibiotic therapy with Gram-negative spectrum, since the germs involved are intra-abdominal, aminoglycosides, quinolones and even metronidazole are recommended.
Keep gastric protector and anti-emetic fixed until the abdominal frame is relieved.
Surgical treatment
Usually these patients in their acute phase are medically managed and then surgically operated on to perform cholecystectomy (removal of the gallbladder).
Sources:

steemSTEM is a project of the chain of blocks that supports the scientific content in different areas of science. If you want to know more about this wonderful project you can join the server in discord
This article will be published at https://www.steemstem.io/
link
If you have any questions about any topic of medicine or present any disease you can comment the publication or write me in discord and I will attend you.
Dr. Ana EstradaI hope you enjoyed my content.
Hello,
Your post has been manually curated by a @stem.curate curator.
We are dedicated to supporting great content, like yours on the STEMGeeks tribe.
If you like what we are doing, please show your support as well by following our Steem Auto curation trail.
Please join us on discord.
Thank you @stem.curate
This post has been voted on by the SteemSTEM curation team and voting trail. It is elligible for support from @curie and @minnowbooster.
If you appreciate the work we are doing, then consider supporting our witness @stem.witness. Additional witness support to the curie witness would be appreciated as well.
For additional information please join us on the SteemSTEM discord and to get to know the rest of the community!
Thanks for having used the steemstem.io app and included @steemstem in the list of beneficiaries of this post. This granted you a stronger support from SteemSTEM.
Thank yo very much @steemstem
According to the Bible, What does the Bible say about changing religions? (Part 2 of 2)
Comment what you understand of our Youtube Video to receive our full votes. We have 30,000 #SteemPower. It's our little way to Thank you, our beloved friend.
Check our Discord Chat
Join our Official Community: https://beta.steemit.com/trending/hive-182074