THE PROSTATE A PROBLEM FOR MEN?
THE PROSTATE:
The prostate is the organ that is most frequently affected by diseases in men over fifty years. The prostate is a gland present only in the male sex, located below the bladder.
WHAT IS PROSTATE?
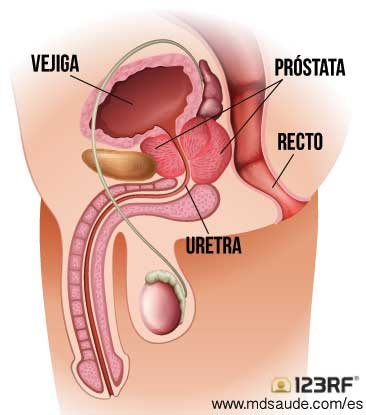
The prostate is a gland, present only in the male sex, located immediately after (below) the bladder, before the start of the penis and in front of the rectum. The urethra, the channel that carries urine from the bladder to the outlet of the penis, passes inside the prostate as if it were a tunnel inside a mountain.
The prostate has a size of approximately 3 cm in diameter and 15-20 grams in weight. It is part of the male reproductive system, being responsible for the secretion of a fluid that protects the sperm from the acidic environment of the vagina and increases its mobility, facilitating the arrival of the same to the ovule.
SYMPTOMS OF PROSTATE

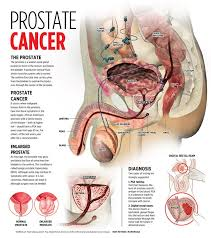
The three main diseases of the prostate, prostate cancer, benign hyperplasia and prostatitis cause similar symptoms that are a product of their anatomical characteristics.
Any increase in the volume of the prostate is sufficient to cause compression of the urethra, leading to the most common symptoms, such as a weak urinary stream and difficulty in starting to urinate.
The compression of the urethra is also responsible for another very frequent symptom: nocturia, which is the need to urinate several times during the night.
The patient needs to urinate at dawn because he can not completely empty his bladder, so it fills up faster. When the bladder is full, it gains enough strength to overcome the obstruction caused by the enlarged prostate. However, when the amount of urine begins to decrease, there is no longer enough pressure to overcome this barrier and the patient stops urinating even when they have some volume of urine in the bladder.
Other common symptoms of urethral compression are the sudden need to urinate, the urge to urinate but not getting it and interruptions while urinating. All these symptoms fit into the term prostatism. Most patients with prostatism have hyperplasia of the prostate, but the diagnosis of cancer should always be ruled out.
If the prostate grows a lot, there may be a total obstruction of the urethra, which leads to the retention of urine. When the urine fails to be drained from the bladder, it eventually returns to the kidneys, a condition called hydronephrosis. This is a complication that causes kidney failure and, if not corrected in time, can evolve with permanent damage to the kidneys.
WHAT PROBLEMS AFFECT THE PROSTATE?
The three diseases that develop most frequently from the prostate are:
Benign Prostatic Hyperplasia (benign growth)
Prostate cancer (malignant growth)
Prostatitis (infection)
It is important to make a correct differential diagnosis to indicate the appropriate treatment. In men younger than 50 years, the most frequent problem is prostatitis. In men older than 50 years, the most frequent disease is Benign Prostatic Hyperplasia (BPH). Although it is less frequent, the development of a prostate cancer can occur and it is important to diagnose it early (localized) and offer a curative treatment.
CANCER IN THE PROSTATE
WHAT IS PROSTATITIS?
It is an inflammation of the prostate usually caused by a bacterial infection. It is very common and affects almost half of men at some point in their lives.
We can distinguish different types of Prostatitis:
Acute Bacterial Prostatitis: it presents with high fever, intense micturition discomfort (a lot of frequency, urgency and itching) and sometimes difficulty urinating.
Chronic Bacterial Prostatitis: usually occurs with repeated episodes of Urinary Infection (frequency, urgency and tingling) and between episodes may not have any symptoms or present a sustained clinical history of chronic pelvic pain.
Chronic Pelvic Pain Syndrome. There are 2 types:
Chronic Inflammatory Pelvic Pain Syndrome
Chronic Non Inflammatory Pelvic Pain Syndrome
Asymptomatic Inflammatory Prostatitis
WHAT IS BENIGN PROSTATIC HYPERPLASIA?
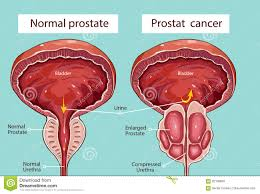
The prostate gland tends to grow with age and from 40-45 years the prostate can grow rapidly leading to benign prostatic hyperplasia (BPH). BPH can compress the urethra and is responsible for the appearance of urinary symptoms (problems urinating) in most men over fifty years.
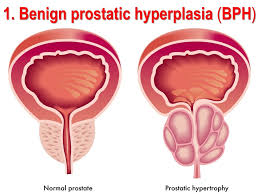
In the image we observed how the growth of the central area of the prostate produces compression of the urethra making it difficult to empty the bladder, raise the bladder floor and hypertrophy of the bladder muscle (detrusor). These circumstances are what cause the symptoms that we expose below.
WHAT SYMPTOMS DOES BPH PRODUCE?
The growth of the prostate can produce symptoms that we call irritative:
Urinating more frequently (frequency)
Get up at night to urinate (nocturia)
Having to go quickly to the toilet when you feel like urinating (urge to void)
And in severe cases, escape of urine
And symptoms that we call obstructive:
Decreased strength and voiding (weak and slow flow)
Sometimes, gagged voiding caliber or micturition at various times
Difficulty and need to use force to start urination
Drip at the end of urination
Feeling incomplete emptying of the bladder
Sometimes urine retention (inability to urinate)
These imitative or obstructive symptoms are usually associated and in general they are evolutionary, that is, they get worse.
In some patients part of the urine is retained in the bladder (residual urine). When this process progresses, there is a distension of the bladder and then an affectation of the high urinary tract (ureters) and the kidney that can lead to renal failure.
WHAT FACTORS FAVOR PROSTATE CANCER?
First, age. Prostate cancer usually occurs after age 50 and its frequency increases with age.
Family history: males with a father or siblings who have suffered prostate cancer have a risk three times higher. If there are 3 affected males in the same family, the risk is 10 times higher. If family members who have had prostate cancer have had it at a young age (45, 50, 60 years), the risk of prostate cancer is higher for males in the family.
Race: African-Americans have the highest risk of prostate cancer. Below are the whites and Hispanics. Asians are the least at risk for prostate cancer.
Food: Prostate cancer is more common in men with a high-fat diet.
WHOM TO GO TO TO CHECK MY PROSTATE?
The doctor who specializes in prostate problems is the urologist.
In men over 45 years old:
Whether or not there is prostate cancer
- If the growth is benign, what clinical symptoms it produces in the patient and if a treatment is necessary
- How the prostate affects sexuality
- How the erection works
- The level of sexual desire

WHAT PROOFS ARE CARRIED OUT TO REVIEW THE PROSTATE?
The revision or prostate check is simple but must be done well, in a personalized way and in a confidential environment.
It is mandatory to carry out a good clinical history by an experienced urologist, dedicating the necessary time for the patient to tell us all their prostate, sexual problems, etc ... The clinical history must be completed with a good physical examination of the kidneys, abdomen , bladder, testicles and especially the prostate.
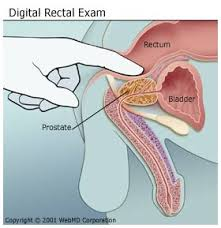
The realization of a digital rectal examination allows to assess the size of the prostate and detect if there are hard nodules suggestive of cancer. This rectal examination does not have to be annoying if the urologist does it with care and without haste.
In addition, the basic revision of the prostate should include a blood test, determining PSA (Specific Prostate Antigen) and creatinine, (kidney function) and a urinalysis.
In certain patients, it may be advisable to perform other tests: Nuclear Magnetic Resonance (MRI) of prostate, 4Kscore in blood, PCA3 in urine, ultrasound, flowmetry, voiding residue, etc. The urologist must decide which patients need these tests.
HOW TO DIFFERENTIATE BETWEEN BENIGN GROWTH AND PROSTATE CANCER?
The initial diagnosis will be based on the determination of PSA (specific prostate antigen) and a Rectal Touch made by an expert urologist.
PSA is a more prostate-specific marker than cancer-specific, which makes it imperfect. For example, PSA may be elevated in patients without prostate cancer, but who have a large prostate with benign prostatic hyperplasia, or in patients with prostatitis or urine infection.
There are no "magic" levels of Total PSA that allow us to ensure that a man is not at risk of developing prostate cancer. In general we consider normal a total PSA figure below 4 ng / ml, but PSA levels should be assessed individually and other factors analyzed (age, family history, digital rectal examination, prostate size).
In addition to the total PSA, we have a fraction called free PSA that allows us to calculate the quotient that results from dividing the free PSA by the total PSA. The higher the free PSA / total PSA ratio the more likely it is for a benign growth (HBP). Conversely, when the free PSA is low and the total PSA is high (free PSA ratio / low total PSA) the greater the probability of prostate cancer.
In doubtful cases we can assess the PSA velocity (as it has been increasing over time) and the so-called PSA density (it consists in dividing the PSA by the volume of the prostate.
We also have more specialized tests: Nuclear Magnetic Resonance (MRI) of the prostate and the 4Kscore test that is performed in a blood test. See section: Avoid prostate biopsies.
A well-performed Nuclear Magnetic Resonance (MRI) (expert radiologist) can detect the presence of suspicious areas of prostate cancer (PIRADS 4, PIRADS 5) and in these cases an MRI-ultrasound fusion biopsy should be considered (See section: Avoiding biopsies of Prostate).
Finally, in patients with suspected prostate cancer (elevated PSA, suspicious digital rectal examination, MRI with suspicious areas of prostate cancer, the definitive test that confirms the presence of prostate cancer is a prostate biopsy.
WHAT IS PROSTATE BIOPSY?
1- Transrectal biopsy guided by ultrasound (classical technique)
Guided by ultrasound, we puncture the prostate through the rectum to take 12 to 18 small fragments of different areas of the prostate. The ultrasound image does not distinguish suspicious areas of cancer. With this classic technique a mapping of the prostate is performed, but prostate cancer can exist in non-biopsied areas.
2- Perineal biopsy guided by fusion of MRI and ultrasound.
Initially a prostate magnetic resonance is performed and if suspicious areas are detected, the patient is offered a prostate biopsy guided by magnetic resonance.
Perineal biopsy guided by Fusion NMR-ECO gives us much more accurate information about the suspicious areas of prostate cancer that we must biopsy. The 59% of men who had previously had 2 or more biopsies and had negative results (biopsies with the classic technique), when performing a perineal biopsy guided by fusion, were diagnosed with cancer.
HOW MUCH TIME SHOULD I CHECK?
All men over 45 years old should consult their urologist once a year.
In men with a family history of prostate cancer and vasectomized prostatic revision should begin at 40 years
HOW CAN BENIGN PROSTATIC HYPERPLASIA BE TREATED?
Extracts of plants (Phytotherapy).
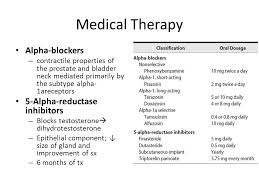
Alpha-blockers: are drugs that relax the smooth muscle of the prostate, so that they reduce the compression that the prostate exerts on the urethra and this allows the urine to come out more easily. They improve both irritative and obstructive symptoms. They have few adverse effects (asthenia, impaired ejaculation). They do not reduce the size of the prostate and do not stop the progression of BPH.
Tadalafil 5 mg. It simultaneously improves prostate symptoms and erection in a very important way. It is a very appropriate treatment for patients presenting with BPH and erectile dysfunction.
Inhibitors of 5-alpha-reductase. They are drugs that block the action of 5-alpha-reductase. When this enzyme is blocked Dihydrotestosterone is not produced and this leads to a decrease in the size of the HBP. These medications do slow the progression of BPH but have more frequent adverse effects, mainly decreased sexual desire (20-30%) and erectile dysfunction (10-20%).
Combination treatment (Alpha-blockers + 5-alpha-reductase inhibitors). In patients with large prostates and moderate or severe symptoms, a combination treatment may be indicated. The alpha-blocker offers a rapid improvement in symptoms and the 5-alpha-reductase inhibitor slowly produces a decrease in the volume of the prostate. Studies at 4 years have shown that with this association the size of the prostate decreases by 27% and the need for surgery is reduced by 50%.
TIPS ON YOUR PROSTATE
All men over 45 years should review annually their prostate, erection and sexual desire (Integral Health of the Man). The urologist-andrologist is the most suitable specialist for this complete review.
An adequate prostate revision allows to differentiate between malignant (cancer) or benign (HBP) growth.
Prostate cancer diagnosed early can be cured.
There are very effective medical and surgical treatments for Benign Prostatic Hyperplasia.
The vaporization of the prostate with green laser or plasmokinetic energy is an excellent option to eliminate prostate tissue and produces an immediate relief of symptoms.
Enucleation of HPB with Holmiun Laser is an excellent treatment for large prostates.
In well-located and low-risk prostate cancers Focal Treatment allows only the area of the prostate where the cancer is removed.
SOURCE OF CONTENT:
https://en.wikipedia.org/wiki/Prostate
https://www.webmd.com/urinary-incontinence-oab/picture-of-the-prostate
Thanking you in advance for taking your valuable time and reading this publication. I hope it has been to your liking, soon I will make other publications of other topics of interest. Do not forget to leave a comment, constructive criticism or contributions to this topic and if you liked to give me your favorable vote. They want Steemists. Thanks for your. attention.

Not influenced by religion, ideology, politics or any other kind, just for health. Prostate issues are rising with high intake of meat. You don't have to stop eat meat, but recommended other mild (raw) diet.
Yes, you should eat more fruits and vegetables, for the prevention of this disease and maintain periodic medical control. Thanks for your comment. Regards