THE BEAUTIFUL AND COMPLEX MECHANICS OF BREATHING. EDUCATIONAL POST.
This post is educational for Physicians, nurses, respiratory therapists, patients with lung diseases and needless to say, a very fun post for all. I will talk about the mechanics of how we breathe. You may find this post breathtaking.
Most of us find this topic complex to understand. I have made it as easy as possible.
The structure
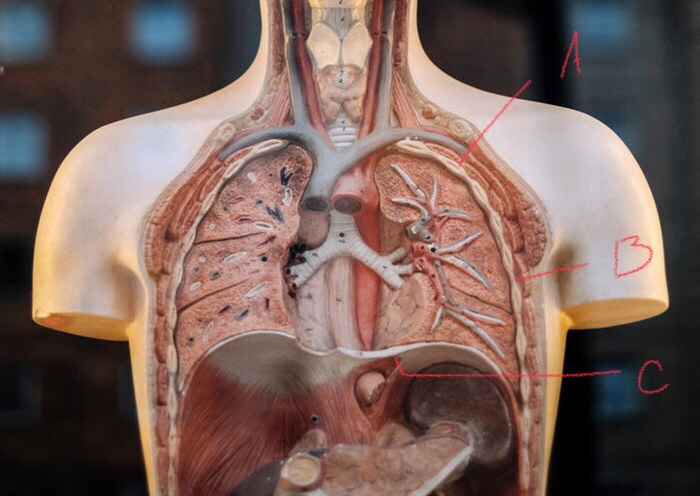
source, modified
A= Rib, B= Intercostal muscle ( muscles between ribs), C =Diaphragm (big muscle of breathing).
There is one more structure that is important in breathing. This is the Pleura. Pleura is a very thin serous membrane that surrounds the lung. It folds upon itself so there are 2 membranes with a potential space between them filled with a very small amount of pleural fluid which serves as a lubricant during chest and lung movements. The membrane that hugs the lung ( inner membrane) is called the visceral pleura and the outer membrane is called the parietal pleura. Imagine double bagging groceries. The structure is somewhat like that ( but not exactly). It just serves to get a mental image. The lungs are the groceries and two bags are the pleural membranes. Here is a neat diagrammatic representation.
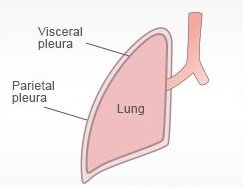
source, modified
Let’s talk about compartments.
To understand how we breathe we need to understand how the above noted system is divided into various compartments and the pressures in those compartments. I will do that in this section. Then I will move to how they all work together like a fine Swiss watch to make it all happen. The diagram below exaggerates the compartments, especially the intrapleural compartment ( space between visceral and parietal pleura) to make understanding easier.
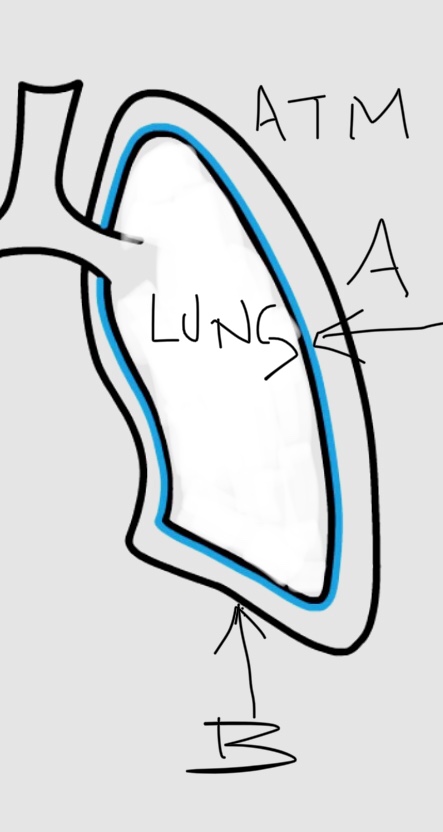
[source,self: A= visceral pleura, B= Pareital pleura, Space between A and B= Intrapleural space]
The atmosphere or air around you is one compartment. Denoted ATM in diagram above.
The lungs are the second compartment.
The third compartment is the space between the pleura called the intrapleural space.
Pressures in the compartments at rest. Numbers are at sea level.
The Atmospheric pressure is 760 mm Hg.
The lung compartment (intrapulmonary pressure) has the same pressure, 760 mm Hg.
The intrapleural compartment, very importantly has a lower pressure of about 756 mm Hg.
How did the pressure in the intrapleural space get to be lower?
It depends on 3 factors namely elasticity of lungs, surface tension and elasticity of the chest wall.
With lung elasticity the tendency of the lungs is to assume a small volume and thus it pulls the visceral pleura away from the parietal pleura. At low lung volumes the surface tension in the lungs is directed inwards due to interaction of water molecules. The tendency of the chest wall is to expand due to various interactions of structures that constitute it. These interactions give a tendency to increase intrapleural space volume thus lowering the pressure.
One thing that will confuse the reader while looking at this subject in various texts is how the pressure values are described. For example, the intrapleural pressure may be called negative and given a value of -4. They are simply taking the atmospheric and lung compartment values as 0. By making atmospheric pressure value 0 as a reference only then then the intrapleural space pressure is -4. So if 760 ( atmospheric and lung compartment pressures) is regarded as 0, then 756 ( intrapleural compartment pressure) is -4. For whatever reason this is how it is often described in literature.
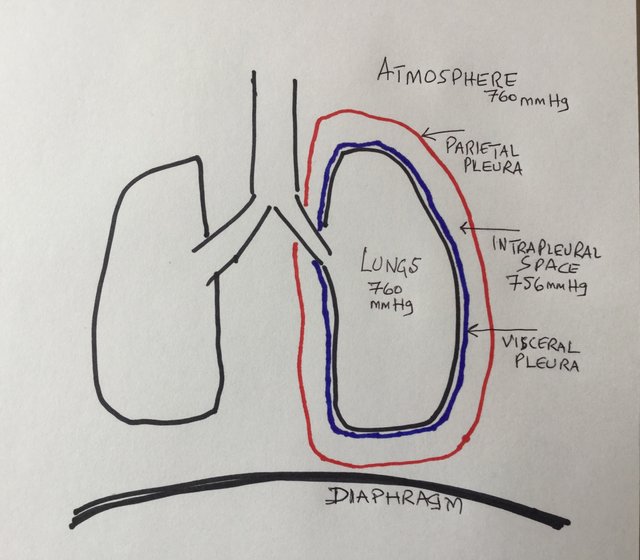
[source,self, diagrammatic exaggerated compartments/pressures at rest]
Process of Inspiration.
The central nervous system sends signals to the intercostal muscles and the diaphragm which are the main muscles involved in breathing. You can read the simple cliff notes here.. My post will focus on lungs primarily. As the central nervous system activates these muscles, it results in the diaphragm doming downwards and the ribs moving upwards and outwards and the sternum ( breast bone) moving outwards. This essentially increases the thoracic volume. How does this help with breathing? We have to go back the compartment pressures and analyze what is going on.
More about pressures.
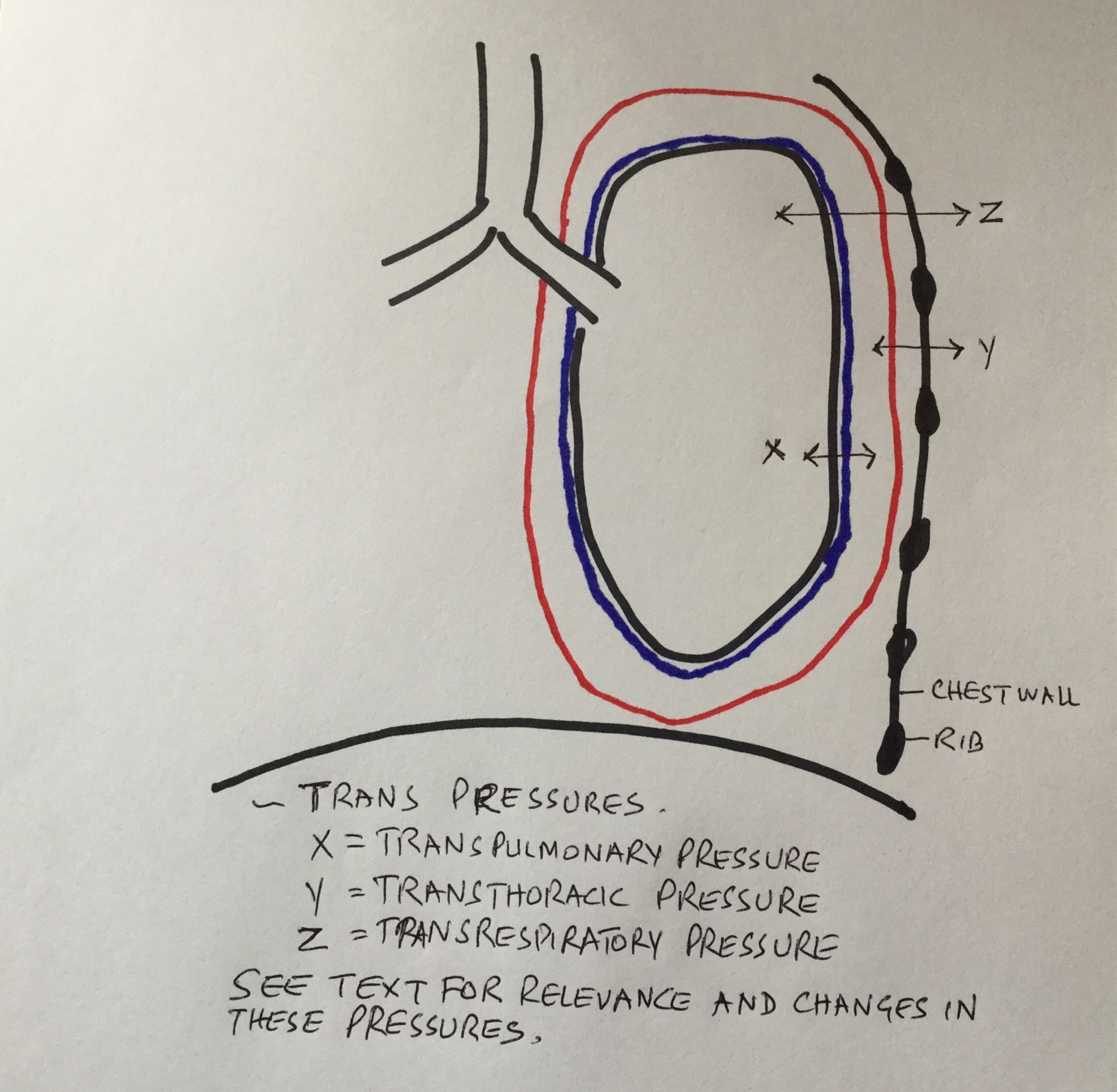
[source,self]
I will introduce 3 new pressures here. The names of these 3 pressures start with ~Trans. It so because these are not compartment pressures alone but how the interaction between these pressures exert forces across the walls of these compartments.
- Transpulmonary pressures is Intrapulmonary pressure - Intrapleural pressure. 0- (-4)= 4
- Transthoracic pressure is Intrapleural pressure - atmospheric pressure. -4- 0= -4
- Transrespiratory pressure is intrapulmonary pressure - atmospheric pressure. 0-0=0
All in mm Hg and all in a state of rest.
Note that Transpulmonary pressure is positive, causing a tendency for lungs to expand. Transthoracic pressure across the chest wall is negative or deflationary.
Air moves between the compartments of the lung and the atmosphere. The transrespiratory pressure is 0. Thus no air exchange happens in a state of rest
let’s see what happens during inspiration.
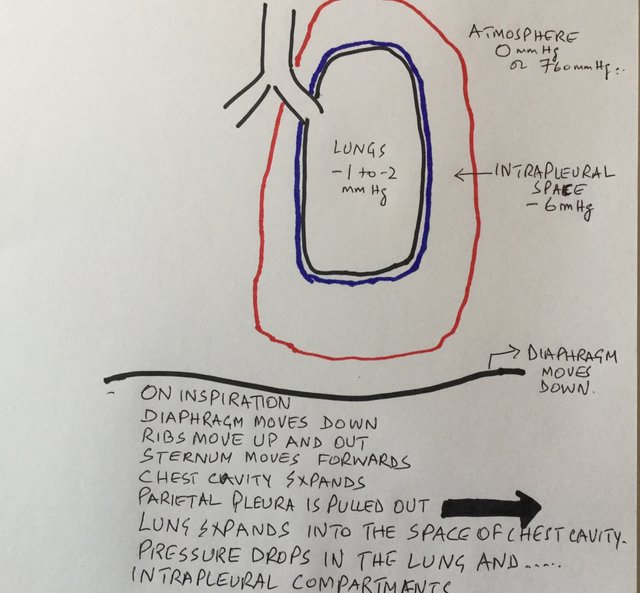
[source,self: pressure changes in compartments during inspiration]
We read in the process of inspiration section how the chest volume expands by the diaphragm coming down and ribs moving upwards and outwards with sternum moving forward. As this happens the space between the visceral pleura and parietal pleura increases. As this volume increases the pressure inside the intrapleural compartment decreases. It was -4 at rest and it drops to -6 mm Hg approximately. The lung now starts to expand into the expanding thoracic cavity. The pressure inside the lung or intrapulmonary pressure drops. It was 0 mmHg at rest and drops to -1 to -2 mmHg. So 2 compartments changed pressure. Third compartment, the atmosphere stays at the same pressure. Let’s see the changes in the ~Trans pressures.
- Transpulmonary pressure is intrapulmonary pressure - Intrapleural pressure. -1-(-6)= 5mmHg.
- Transthoracic pressure is intrapleural pressure - atmospheric pressure. -6- 0 = -6 mmHg.
- Transrespiratory pressure is intrapulmonary pressure- atmospheric pressure. -1-0= -1mmHg.
All these interactions have created a gradient of pressure between the lung and the atmosphere with lower pressure in the lung. Air thus flows from the higher gradient atmosphere to the lower gradient and into the lungs. The flow stops when pressures in both compartments equalize.
The process of exhalation.
All this work just to get in one breath. Now try to imagine reversing the processes and try to make sense of exhalation in your head or on paper. Happy to make another post on exhalation physiology if any clarification is requested in comments.
Notes:
Diagrams are my own. I am obviously not Picasso. Diagrams are exaggerated so the science makes sense.
References:
- https://www.britannica.com/science/human-respiratory-system/The-mechanics-of-breathing
- http://teachmephysiology.com/respiratory-system/ventilation/mechanics-of-breathing/
- OpenStax, Anatomy & Physiology. OpenStax CNX. Feb 26, 2016 http://cnx.org/contents/[email protected]
- https://www.universalclass.com/articles/health/the-physiology-of-breathing.htm
- Murray and Nadel’s textbook of Respiratory Medicine.
- West’s Respiratory Physiology.
Being A SteemStem Member
Hello Ned. What interests you most about pulmonology and respiratory medicine? You have a nice physiology post here that goes through the basics. Good job making it easy to digest for the average reader. Maybe you can explore the physics behind the pressure gradients and how the compliance and elasticity related to the function of the diaphragm in another post. Keep up with the interesting posts!
It happens to be my job. I am a pulmonologist. Be happy to make the other post.
Excellent, I had a feeling you were working in a related field due to the language and description.
I really don't want a Swiss watch inside my body ;)
@Lemouth, perhaps not inside but I can see the Patek on you wrist. Looks really good. Did you know that a small part for Patak is hand perfected and can take upto a year for it to work so perfectly and harmoniously with other parts that the watch will be accurate a 100years later. Accurate not to the second though. By that measure it’s funny how easily biology can make us work so perfectly, life after each life. Makes me wonder how these codes were formed and what are they?
When you guys at CERN find out, I will be waiting in line to get the answers.
Thankyou for looking at my post.
We are not really looking, at CERN, on biology. I am as amazed as you when I learn about this field. There is indeed no connection between CERN and how tour body works.
Note that whatever we will find out at CERN, I will let you (and all other steemians) know :)
Congratulations! This post has been upvoted from the communal account, @minnowsupport, by nedspeaks from the Minnow Support Project. It's a witness project run by aggroed, ausbitbank, teamsteem, theprophet0, someguy123, neoxian, followbtcnews, and netuoso. The goal is to help Steemit grow by supporting Minnows. Please find us at the Peace, Abundance, and Liberty Network (PALnet) Discord Channel. It's a completely public and open space to all members of the Steemit community who voluntarily choose to be there.
If you would like to delegate to the Minnow Support Project you can do so by clicking on the following links: 50SP, 100SP, 250SP, 500SP, 1000SP, 5000SP.
Be sure to leave at least 50SP undelegated on your account.
@nedspeaks great job at making this easy to comprehend. I have no education whatsoever in this field and I still found this article interesting.
I am shocked that you read it without being in the field. Thankyou so much. I am glad that it was easy enough for all.
I can't believe pulmonology and respiratory medicine could be explained in engineering terms until now.
I salute your insightful work. I more than fell in love with your humors too.
Thanks for sharing this. I sure would keep tab on your posts
Thankyou sir, I don’t often blog as I am a full time physician. Your interest will certainly boost my output
Oh I see. So thoughtful of you to still find time to share educative posts like this. You're well appreciated sire